

AAP Staging and Grading
Feb 03, 2023Local anesthesia is most often administered in the hygienist's chair when treating active periodontal disease. Every dental professional is aware of the prevalence of gum disease. We treat it daily and treat it well. But properly charting it seems to still be throwing many of us for a loop. When I teach my local anesthesia course, there is confusion about the correct AAP staging and grading of this disease, and given the current state of insurance denials, it is important to be able to defend your diagnosis to help ensure your patient get the care they need.
AAP Classification System
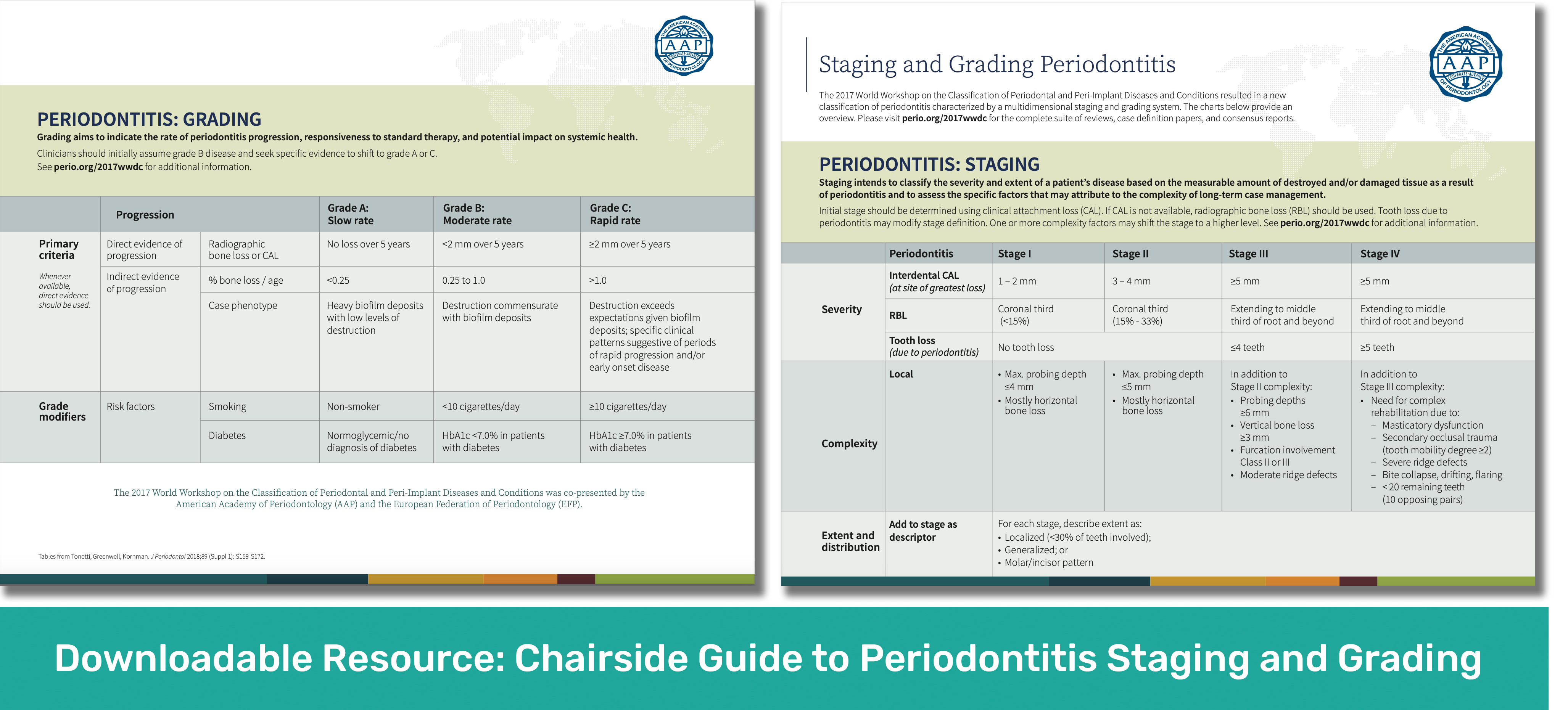
It has been six years since the American Academy of Periodontology created the newest classification system for periodontal disease. Per the AAP, this “new system is characterized by a multidimensional staging and grading system.”
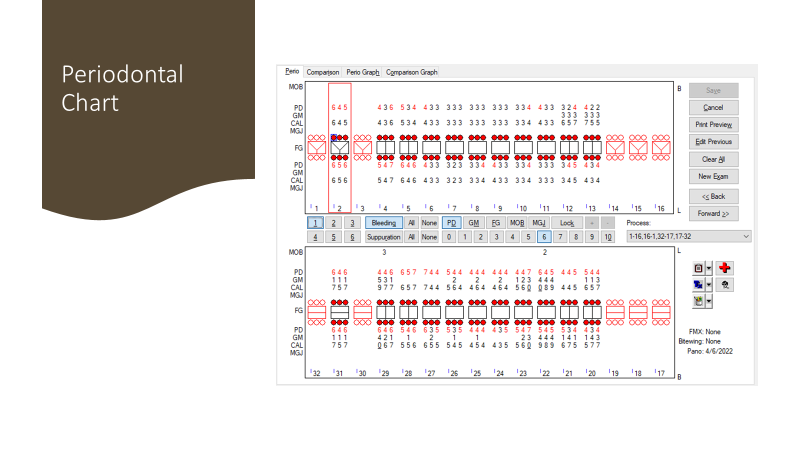
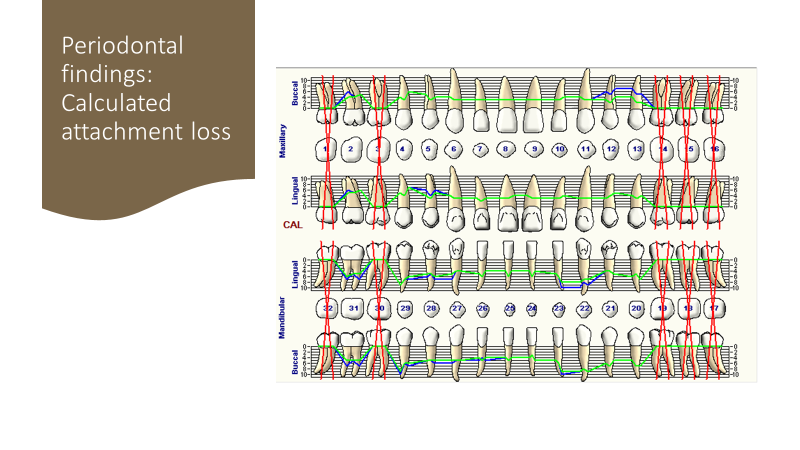
AAP Staging and grading has replaced terms like rapidly progressive periodontitis, necrotizing ulcerative periodontitis, and refractory periodontitis. As always, the hallmark of periodontal disease is calculated attachment loss (CAL). Initial stage of periodontal disease will be determined using clinical attachment loss. Do not believe the denial letters from insurance companies that radiographic bone loss is the hallmark of periodontal disease. IT IS NOT. By the time radiographic bone loss is present, you are likely into stage II periodontal disease.
Using this Classification System in Your Patient Notes
Stage I indicates early periodontal disease. Calculated attachment loss will be 1-2 mm. There may or may not be radiographic evidence of bone loss (RBL). If noted, the RBL will be less than 15% and limited to the coronal third of the tooth. Per AAP, max probe depths will be less than or equal to 4 mm. GOOD LUCK getting insurance coverage with only 4 mm probe depths and little to no radiographic bone loss. This disconnect is part of why we underuse this system of AAP staging and grading. Please do not get discouraged. I often label stage one periodontal disease when there are generalized 5 mm pocketing.
Stage II has RBL of 15-33% of the tooth. You will be able to detect this on radiographs. Per the AAP guidelines, max probe depths will be less than or equal to 5 mm. Again, I have found myself writing multiple appeal letters. I often have localized 6 mm pocketing on patients that I call Stage II.
Stage III has CAL of 5 mm or more. NOT 5 mm pockets–5 mm of attachment loss! This is bad. This is often when I get out my referral pad. RBL extends to the middle third of the root or further. There may be a history of tooth loss due to periodontal disease. You will have probe depths of 6 mm or greater.
Stage IV is really bad. Like stage III, there is a minimum of 5 mm of CAL & RBL extending to the middle third of tooth or further. Unlike stage III, there may be more teeth lost to the disease. Secondary occlusal trauma and tooth mobility are also hallmarks of advanced disease. In my office, this is a direct-to-the-periodontist, "do not pass go." No restorative until we are cleared by the specialist.
I hope your brain is not hurting. If you are not currently using this system, it can feel overwhelming. Good news! Grading of periodontal disease is more straight forward. Our patients will be Grade A, B, or C.
I assume my patients are Grade B unless I find evidence that the disease is potentially more or less aggressive than average. If the disease is aggressive, my patients are moved to Grade C. If they smoke, are pregnant or diabetic, they are grade C. If it is slower than average progression – they can be moved to Grade A. It is rare for me to diagnosis grade A. This is reserved for my patients that clearly have CAL, but no active disease. When in doubt, they are Grade B.
www.perio.org is a great resource. Use it!
Again, I hope you do not become discouraged. While there is a disconnect between this system and insurance coverage, I hope you follow the AAP guidelines.

